Introduction
Human factors investigation procedure
Data collection & occurrence sequence determination
3.1. The circumstances surrounding the accident
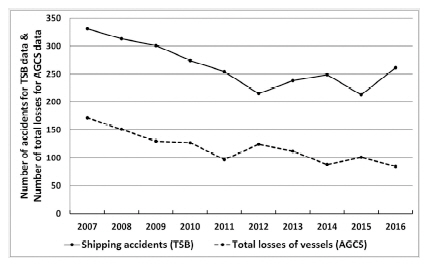
Brief description: In a head-on situation, the northbound Sand pump Carrier (Vessel A) collided with the southbound Tanker (Vessel B) in a visibility of over 3 miles at night. If both vessels had kept their courses and speeds, the collision accident would not have occurred. However, each vessel failed to stand a vigilant watch and did make unsafe decisions and did act unsafely.
3.2. Cognitive process model
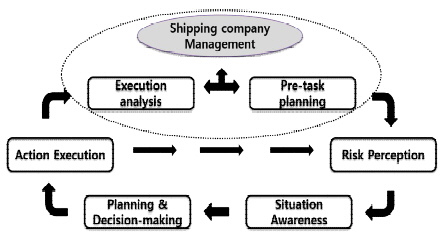
Pre-task planning: plan for the task considering ship’s state, crew member’s ability, task features, external factors, etc.
Risk perception: detect dangerous situations or events that could affect pre-planned normal tasks. Check if a dangerous situation or an event was detected at a proper time, and an appropriate method or system was selected for the detection by the OOW (Officer Of Watch-keeping).
Situation awareness: comprehend the dangerous situation causing a threat to the safety of the vessel based on the operator’s ability and experience. What kinds of methods (including OOW’s knowledge and experience) or systems were used to comprehend the dangerous situation? Check if the OOW understood the situation clearly. If not, what was the reason?
Planning & Decision-making: identify all possible actions that could have avoided the dangerous situation and choose the most appropriate one. Check if all the plans to avoid the dangerous situation were identified properly and if the most appropriate one of them was selected to avoid the dangerous situation. If not, what was the reason?
Action execution: the most appropriate actions must be initiated and performed at the appropriate place and time, and periodic checks should be made to ensure that the action sequence is proceeding as intended. Check if action was taken properly at a proper time. If not, what was the reason?
Execution analysis: analyze the operator’s actions performed and the dangerous situations or events that had occurred.
3.3. Determination of occurrence sequence (case study)
Table 1
① Determine the occurrence sequence (fill the occurrence sequence column);
② Fill the remark column with the important factors / additional information;
③ Identify action executions from the occurrence sequence column;
④ Analyze the actions executed using the cognitive process model; and
⑤ Identify unsafe acts and unsafe decisions or conditions for use in Step 2.
Table 2
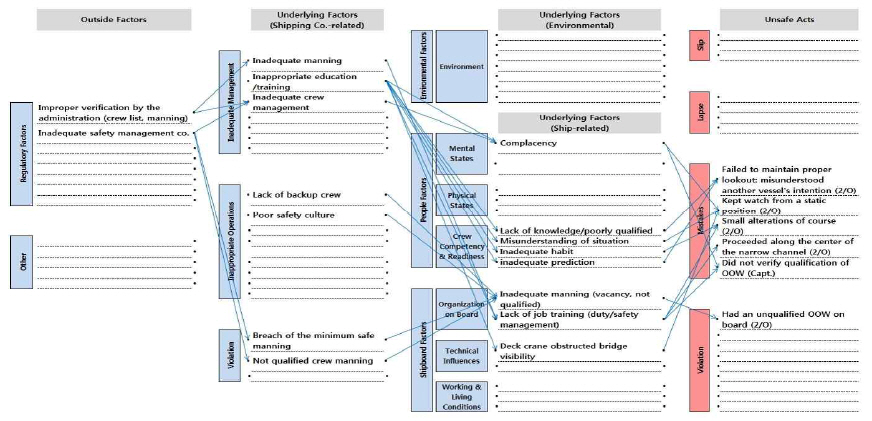
Failed to maintain proper lookout: misunderstood another vessel’s intention / situation (2/O);
Kept watch from a static position (2/O);
Small alterations of course (2/O);
Proceeded along the center of the narrow channel (2/O);
Did not verify the qualification of OOW (Capt.); and
Had an unqualified OOW on board (2/O).
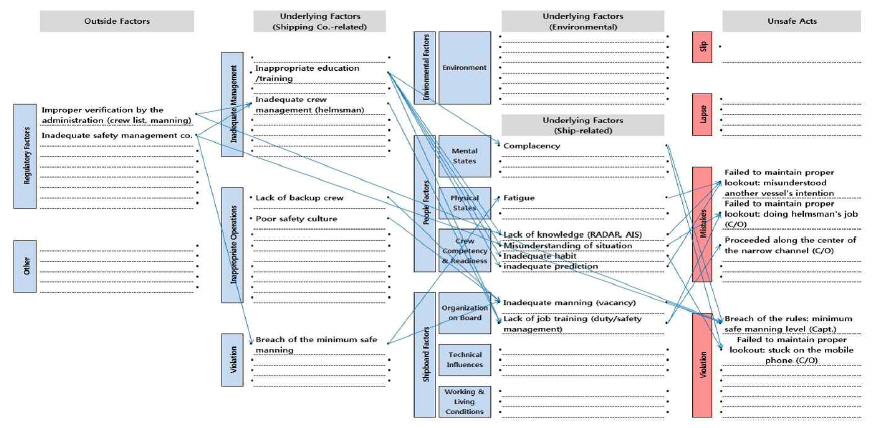
Failed to maintain proper lookout: stuck on the mobile phone (C/O);
Failed to maintain proper lookout: misunderstood another vessel’s intention (C/O);
Failedto maintain proper lookout: doing helmsman’s job (steer the ship) (C/O);
Proceededalong the center of the narrow channel (C/O); and
Breach of the rules - minimum safe manning level (Capt.).
Human factors identification and classification
4.1. Maritime-Human Factor Analysis and Classification System
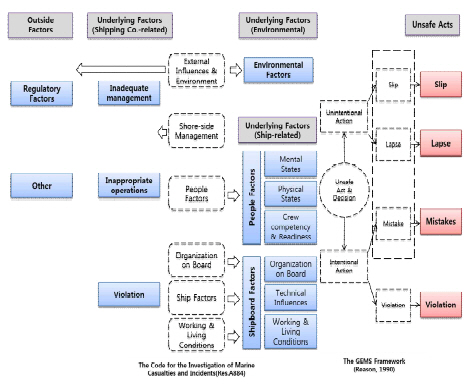
Table 3
4.2. Results of the M-HFACS (case study)
Safety actions development
5.1. Causal chains
5.2. Safety actions identified (case study)
Technical / Engineering: Ergonomic design (equipment, work spaces, man-machine interface etc.), Clear labelling and instructions, etc.
Working environment: Working conditions (noise levels, temperature and humidity, vibration etc.) etc.
Personnel: Training for crew members, Language and cultural issues, Workload, Motivational and leadership issues, etc.
Organizational / Management: Organization policies (recruitment, training, crew levels, etc.), Operational procedures, Safety management systems, etc.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






